
Rural communities across America carry a disproportionate share of chronic disease, yet they receive a fraction of the specialist care available in cities. 20% of the U.S. population lives in rural areas, but only 10% of physicians practice there. That imbalance is not just a geographic quirk. It reflects deep, layered systemic failures in how medicine trains, pays, and supports its workforce. If you make healthcare decisions for a rural community, understanding exactly what drives this gap, and what actually helps close it, is the first step toward building a realistic strategy.
Table of Contents
- Understanding the maldistribution of medical specialists
- Barriers to recruiting and keeping specialists in rural practice
- The logistics of specialist care: travel, coverage gaps, and diagnostics challenges
- Specialist shortages and their impact on rural health outcomes
- Workforce strategies and emerging solutions
- Why conventional solutions alone can't close the rural specialist gap
- Explore healthcare solutions for your rural community
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Specialist shortages in rural areas | Remote communities have far fewer specialist doctors per capita than urban ones. |
| Multiple barriers beyond location | Professional, logistical, and lifestyle factors discourage specialists from rural practice. |
| Diagnostics and travel challenges | Limited local testing and long travel distances worsen specialist access in remote areas. |
| No single solution | Closing the rural specialist gap requires multi-layered community, workforce, and infrastructure strategies. |
Understanding the maldistribution of medical specialists
The word "maldistribution" gets used a lot in health policy circles, but its meaning is concrete: too many doctors are concentrated in wealthy urban and suburban areas, while rural populations go without. This is not simply because rural towns are far from medical schools. It is because the entire pipeline from training to practice to career development favors urban environments at every turn.
"Medical deserts form where specialist access lags far behind community need, leaving patients without timely diagnosis or treatment for serious conditions."
Research on workforce distribution disparities shows that specialist scarcity is not random. It follows patterns tied to income, infrastructure, and historical underinvestment. Rural communities typically suffer the most because they lack the institutional pull of teaching hospitals or large health systems that attract specialists naturally.
The table below shows how dramatically specialist density drops outside urban centers, based on rural versus urban specialist supply data:
| Specialty | Urban (per 100,000) | Rural (per 100,000) | Gap |
|---|---|---|---|
| Cardiology | 9.8 | 2.6 | 73% lower |
| Neurology | 6.4 | 1.1 | 83% lower |
| Oncology | 8.1 | 2.2 | 73% lower |
| Pulmonology | 4.3 | 0.9 | 79% lower |
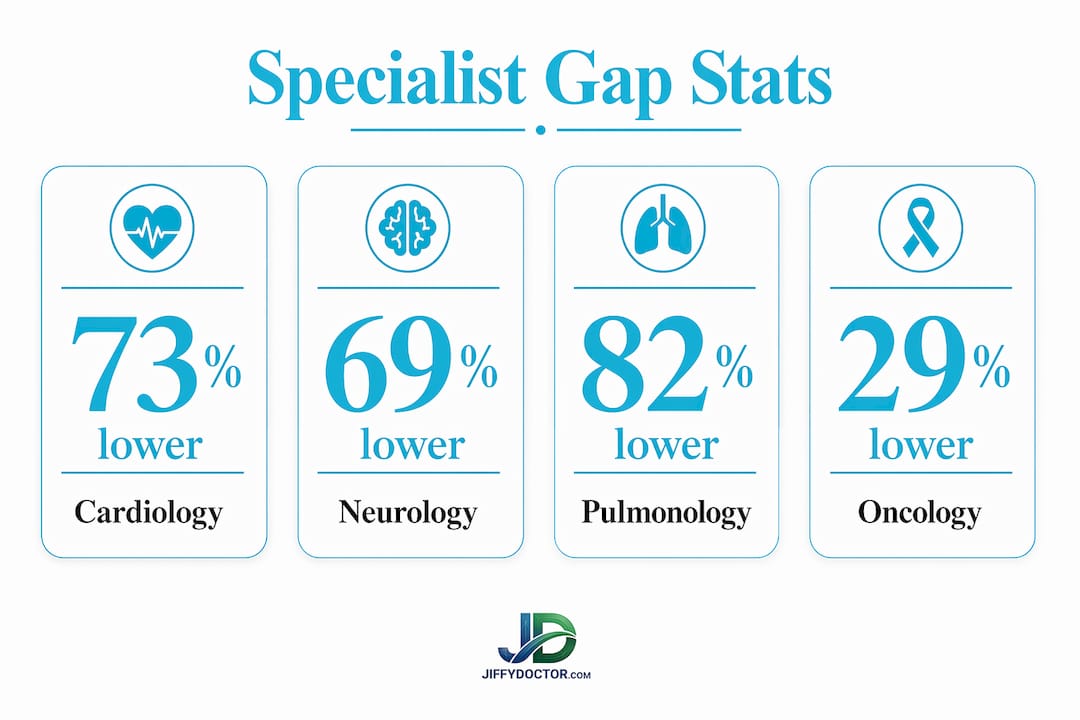
These numbers are not just statistics. They represent real patients who have a heart attack and wait hours for cardiology consultation, or a cancer patient who drives three hours to see an oncologist. For rural healthcare leaders, this table should anchor every workforce conversation you have.
Barriers to recruiting and keeping specialists in rural practice
Understanding why the gap exists requires looking beyond salaries and bonuses. The WHO guideline on health workforce development makes clear that recruitment and retention are difficult because rural and remote practice offers fewer professional opportunities and less stable staffing structures. That instability creates a feedback loop: one specialist leaves, the workload doubles for those who remain, and the next person burns out faster.
Here are the main barriers rural health systems face when trying to attract and hold specialists:
- Limited career growth. Specialists in rural settings rarely have access to advanced research, subspecialty peers, or academic promotion pathways.
- Professional isolation. Without colleagues in the same field nearby, clinical decision-making becomes lonely and stressful.
- Family and partner barriers. Spouses and partners of recruits need jobs too. Rural areas often lack opportunities in law, finance, or other professional fields.
- Burnout from overextension. When one neurologist covers a four-county area, the call burden becomes unsustainable within two or three years.
- Unstable staffing cycles. When a specialist vacancy goes unfilled for months, it disrupts continuity of care and drives patients to seek care elsewhere, which erodes the patient volume that justified the position in the first place.
Burnout and professional isolation drive retention failures in rural settings more than most administrators admit. Many hospitals focus their energy on recruitment packages while underinvesting in the day-to-day experience of doctors already on staff.
Pro Tip: Before you spend another dollar on a recruitment bonus, survey your current specialists about their biggest frustrations. Fixing those first will do more for long-term retention than any signing incentive you can offer.

Financial incentives attract attention, but they do not build loyalty. A cardiologist who moves to a rural community for a $50,000 bonus and finds themselves isolated, overworked, and unsupported will leave when that contract expires. Retention requires building a professional community, not just filling a slot.
The logistics of specialist care: travel, coverage gaps, and diagnostics challenges
Even when a rural health system recruits a specialist, logistical realities can neutralize the benefit. Logistical and travel burdens, along with limited diagnostics, reinforce specialist access gaps in ways that workforce solutions alone cannot fix.
Rural communities typically rely on a mix of the following care delivery models to manage specialist demand:
- Full-time, locally based specialists. Rare outside larger rural hospitals; provides the best continuity but hardest to sustain.
- Visiting specialists. A cardiologist who flies in once a month creates scheduling backlogs and zero availability for urgent cases.
- Telehealth consultations. Growing in availability and effectiveness for many conditions; limited when physical examination or local diagnostics are required.
- Referrals to urban centers. Common and necessary, but costly, time-consuming, and associated with patient no-shows.
- Primary care-led management with specialist support. Effective in systems with strong communication channels, but burdens general practitioners and demands strong upskilling.
The role of telehealth options is real and growing, but decision-makers need to be clear-eyed about its boundaries. A neurologist can review an MRI remotely, but only if the rural facility has an MRI machine and a trained technologist to operate it. A pulmonologist can consult via video, but only if spirometry data is available. The technology is only as useful as the diagnostic infrastructure behind it.
| Care model | Continuity | Cost | Urgency fit | Diagnostic dependency |
|---|---|---|---|---|
| Full-time local | High | High | Excellent | Low |
| Visiting specialist | Low | Moderate | Poor | Moderate |
| Telehealth | Moderate | Low | Moderate | High |
| Referral to urban center | Moderate | High | Poor | Low |
| Primary care led | Moderate | Low | Moderate | Moderate |
Travel burdens deserve more attention than they usually get. When a rural patient misses an oncology appointment because they cannot afford gas or cannot take a day off work, that is not a patient compliance problem. It is a system design problem. Late diagnoses and advanced disease at presentation follow directly from these missed connections.
Specialist shortages and their impact on rural health outcomes
The consequences of specialist scarcity are measurable, not theoretical. Rural supply per 100,000 population includes only 2.6 cardiologists, 1.1 neurologists, 2.2 oncologists, and 0.9 pulmonologists. Compare those figures with urban densities and the mortality math is grim.
Rural Americans die of heart disease, stroke, cancer, and respiratory illness at significantly higher rates than urban residents. Not because rural people are inherently less healthy, but because they receive later diagnoses and less intensive treatment. A patient who sees a cardiologist within 48 hours of a cardiac event has dramatically different outcomes than one who waits three weeks for a telehealth consult.
The most visible consequences of these shortages include:
- Delayed diagnosis. Without accessible specialists, primary care doctors carry conditions beyond their scope and diagnosis timelines stretch dangerously.
- Advanced disease at presentation. Cancer, in particular, is routinely caught at later stages in rural areas because oncology access is sparse.
- Higher financial burdens. Travel, accommodation, and time off work for specialist visits in distant cities create financial strain that causes patients to delay or skip care entirely.
- Fragmented care coordination. When patients shuttle between a rural primary care doctor and an urban specialist, nobody has a complete clinical picture.
- Mental health consequences. Chronic illness managed poorly creates secondary anxiety and depression, and rural mental health specialist supply is even thinner than physical health.
For healthcare leaders in rural communities, these consequences are not abstract. You see them in your emergency department data, your readmission rates, and the conversations you have with primary care staff who are stretched beyond their training.
Workforce strategies and emerging solutions
Given the depth of the problem, it is tempting to look for one big fix. There is none. But there are strategies that, when layered together, can genuinely move the needle.
Financial incentives and education support are commonly used, but evidence for their durability is mixed, especially for specialists. Loan repayment programs and rural training scholarships help build pipeline, but they take a decade to show results. You need short and long-term strategies running in parallel.
Effective approaches to consider:
- Build rural residency programs. Physicians who train in rural settings are far more likely to practice there long-term. If your region lacks a residency program, partnering with a university to create one is a multi-decade investment with proven returns.
- Invest in diagnostic infrastructure. Addressing last-mile diagnostic capacity is essential for specialists whose work depends on imaging, lab results, and monitoring equipment. A telehealth cardiology program without an echocardiogram machine is only half a solution.
- Develop telehealth with real support. Telehealth works best when rural staff are trained to conduct examinations that remote specialists can interpret. That requires protocols, training time, and technology investment beyond just a video platform.
- Create peer networks for rural specialists. Scheduled virtual peer consultations, access to continuing medical education, and connections to academic centers reduce the professional isolation that drives turnover.
- Partner with communities, not just hospitals. Specialists who feel welcomed by the broader community stay longer. Housing support, school quality, cultural fit, and social integration all factor into the decision to stay or leave.
- Leverage evidence-based care accessibility models. Collaborative care frameworks that embed specialist oversight within primary care settings can extend reach without requiring full-time specialist presence.
Pro Tip: Layer your strategies across three timeframes: immediate (telehealth and visiting specialists), medium-term (diagnostic infrastructure and peer networks), and long-term (training pipeline and community integration). A rural health system that only plays one timeframe will always be reacting to crises.
Why conventional solutions alone can't close the rural specialist gap
Here is the uncomfortable reality: most rural health systems approach specialist shortages the same way every year. They post a job, offer a bonus, and hope for the best. When that fails, they add telehealth. When that partially works, they call it solved.
What this approach misses is the cultural and systemic context that makes rural medicine fundamentally different from urban medicine. Specialists are not just employees. They are professionals with complex personal lives, career ambitions, and social needs. A rural hospital that treats specialist recruitment like a logistics problem will keep losing to urban hospitals that offer more of everything.
The deeper issue is that American medical training is built around urban academic centers. Medical students rotate through massive university hospitals. Residencies expose them to high-volume, high-technology environments. By the time a cardiologist finishes training, they have spent a decade acclimating to a world that rural practice cannot replicate. Asking them to leave that world is a significant cultural ask, not just a geographic one.
What we believe rural healthcare leaders genuinely need is a shift in how they frame the problem. Stop asking "how do we recruit more specialists?" and start asking "how do we build a system where specialists can thrive?" That means working with city planners, school boards, and local employers, not just HR departments. It means investing in the social infrastructure of rural communities, not just the clinical infrastructure.
Telehealth is a powerful tool, not a substitute for a workforce strategy. Financial incentives are useful, not transformative. What actually moves outcomes is a sustained, multi-stakeholder commitment to making rural practice professionally and personally sustainable over a career.
Explore healthcare solutions for your rural community
Closing specialist gaps requires both long-term strategy and immediate access tools that work today. For rural communities navigating these shortages, virtual care platforms offer a practical way to extend the reach of available providers and reduce the burden on overtaxed rural staff.
JiffyDoctor connects patients with licensed healthcare professionals through fast, accessible virtual consultations, reducing the friction that keeps rural residents from getting timely medical guidance. For healthcare leaders looking to layer telehealth into a broader access strategy, exploring platforms designed for efficiency and accessibility is a concrete next step. Whether you are looking to improve care coordination or expand the range of services your community can reach, virtual consultation options offer a scalable complement to your existing workforce efforts.
Frequently asked questions
What are the main reasons specialists avoid rural practice?
Specialists are deterred by fewer professional opportunities, professional isolation, challenging staffing cycles, and limited access to advanced diagnostics in rural areas.
How do rural hospitals manage specialist shortages?
They rely on a mix of intermittent visiting specialists, referrals, telehealth, and empowering primary care doctors with remote specialist support.
What specialty areas are most affected by rural shortages?
Cardiology, neurology, oncology, and pulmonology have the lowest per-capita rural presence, with pulmonology at just 0.9 per 100,000 rural residents.
Does telehealth fully solve the specialist shortage in remote areas?
Telehealth improves access significantly, but it cannot replace specialists who require in-person examination or procedures, particularly where local diagnostic capacity is limited.
What can rural health systems do to attract more specialists?
Combining financial incentives with education support, rural training pipelines, improved diagnostics, and community integration gives the best chance of attracting and keeping specialists long-term.